Labrador Health Testing
Why Health Testing?
DNA Testing
We are so lucky in our breed that diseases such as PRA (Progressive Retinal Atrophy), EIC (Exercise Induced Collapse) and HNPK (Hereditary Nasal Parakeratosis ) are now able to be eliminated in our breed due to DNA tests that have been developed for our breed along with a swag of other tests that ORIVET labs have testing for.
All our dogs have a full panel of DNA tests done - we do not rely on clear by parentage testing (CBP) only! We will only use stud dogs who have been DNA tested also. Very rarely, some clear tests have been shown to be in error, so this is why we will never rely on CBP only. Ultimately, all our dogs will be clear, but we do not discard dogs in our breeding program just because they may be a carrier - the DNA tests enable us to keep carriers and make sure we only breed to a clear dog to ensure any resulting progeny cannot be affected by the disease.
Hip and Elbow Scoring - CHEDS scheme
Since the year 2000, all Labrador Retrievers have been required to be hip and elbow xrayed and scored to enable resulting progeny to be registered in Australia.
Hips are scored from 0-53, while elbows are 0 - 3. A cut off limit has not been enforced on higher scores, however, I will not breed any of my dogs with scores more than 1:1 for elbows and then only to 0:0 dogs. It is very frustrating when scores are 0:0 for generations in elbows and an elbow score happens or worse elbow dysplagia happens in a puppy. We cannot guarantee that a puppy will not develop elbow dysplagia as there are lots of complex genes involved and how you look after your puppy can contribute to this also.
Hip dysplagia rarely happens in pedigree purebred Labradors these days. Once again the lower the hip score the better, with the score of 7 the current breed average. I follow the advice given to me many years ago by a very experienced UK breeder - never breed more than a combined total of 20 of the dog and bitch.
In Australia, in 2016 a new sheme replaced the old AVA scheme and the CHEDS scheme (Canine Hip and Elbow Dysplagia Scheme) was initiated and run by the ANKC. The CHEDS scheme has 3 specialist vets who are the only qualified vets to have xrays submitted to them for scoring. In the future it is hoped this scheme registered on the ORCHID database will be an open register for anyonel to view individual dogs scores that have been submitted.
Hip & Elbow Dysplasia are inherited developmental abnormalities in a dog’s elbow or hip joint. The hip/elbow scoring scheme only scores the parents hips and elbows for abnormalities, but does not prevent it being passed onto its progeny. We cannot test for the gene(s) that carry this health issue as below:
Quote from the Victorian Government Code of Practice for the Responsible Breeding of Animals with Heritable Defects that cause Disease:
"Polygenic disease – where more than one gene is involved and environmental effects can add to the severity of the condition. While the following diseases are not listed in the Schedule of the Act they are examples of diseases in this grouping that have widely divergent signs – canine hip dysplasia and elbow dysplasia. These are also conditions where simple and/or effective DNA tests are unlikely to be developed"
Our Labradors are hip/elbow scored after the age of 1 year old. The procedure is performed by a registered veterinarian. The dog’s hips and both elbows are x-rayed in an extended position. The x-rays are then sent to an accredited radiographer to interpret the results – being the ‘score’.
|
The following article explains the disease and how breeders can work towards decreasing the problem. It was written by Dr Wyburn who was the leading specialist in this field for many years. We used Dr Wyburn until ill health forced him to retire. We then sent our xrays to Dr Rawlinson who assisted Dr Wyburn. The AVA then decided to retire from the scheme and now we have the CHEDS scheme run by the ANKC and we chose Dr Makara to continue with maintaining consistency in scoring. HIP AND ELBOW DYSPLASIA DR. R S Wyburn BVMS. DVR. PhD, FACVSc. MRCVS. OVERVIEW Canine hip dysplasia (HD) is a genetic disease which is inherited in a rather complex manner because it is influenced by more than one gene.
Obviously the ideal situation would be to breed only with dogs that have a 0 score. However this is unacceptable as doing so could exclude most if not all of the breed. A compromise has to be reached which will allow the retention of sufficient breeding Such a control programme can be taken a step further by recording the hip status of offspring so that it can be determined which sires are tending to reduce the hip scores of their progeny.
THE SCORING SYSTEM HIP SCORE
The 9 items listed on the scoring sheet are all details of the anatomy of the hip joint that can be seen on an x-ray film. Of these features 8 are scored out of 6 with 0 being normal.
THE GRADING SYSTEM There is not a direct relationship between scoring and grading which causes considerable confusion.
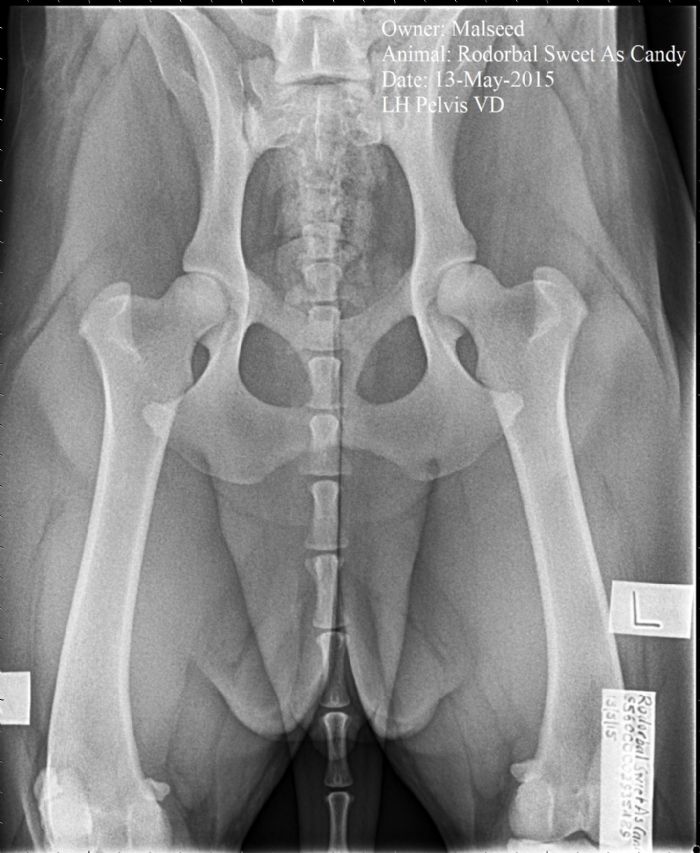
HIP DYSPLASIA The hip joint is a ball and socket joint with the ball (femoral head) being on the proximal end of the thigh bone (femur) and the socket (acetabulum) being on the pelvis. If the hip joint is normal the ball is a neat fit in the socket. Hip dysplasia in itself does not commonly cause lameness. With dogs that have HD the ball is not a neat fit in the socket so the joint is subject to excessive wear and tear. This excessive wear and tear results in the development of degenerative joint disease (arthritis). It is the arthritis that causes the lameness. Other factors can impact of the degree of wear and tear the joint is subjected to.
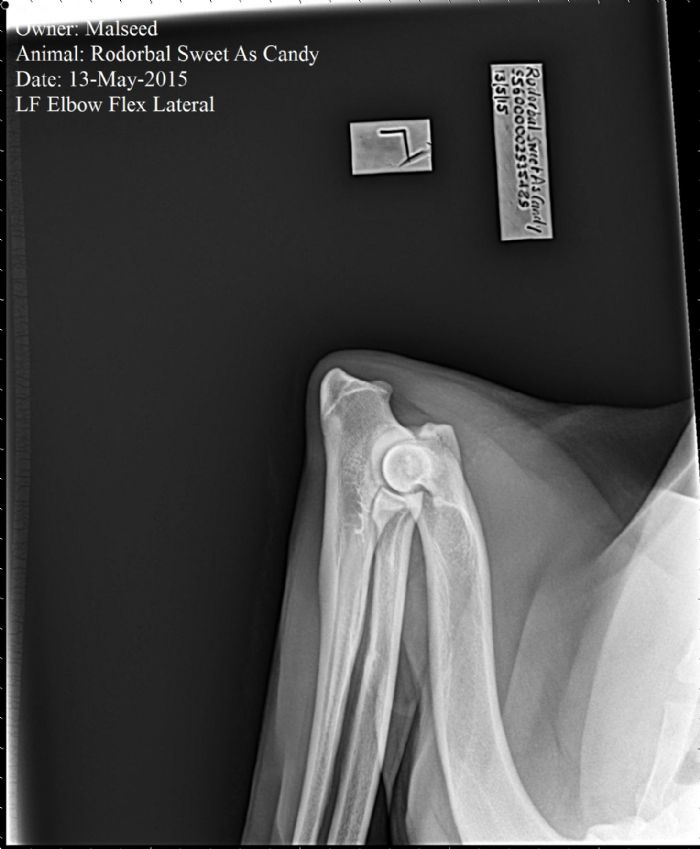
ELBOW DYSPLASIA Elbow dysplasia is a disease with a high inherited component, which primarily affects intermediate and large breed dogs. DEVELOPMENT The elbow joint is composed of three bones (radius, ulna, and humerus) which must all grow together and fit perfectly. The radius and ulna are paired bones with the radius being the main weight bearing bone. The height of the step may vary from barely noticeable to 4 mm or more. When this occurs the weight bearing force on the ulna is increased, resulting in excessive pressure on the medial coronoid process. This leads to fragmentation of the coronoid process. This usually occurs between 5 and 7 months of age. CLINICAL SIGNS Affected dogs are frequently lame or have an abnormal gait. The gait is often characterized by excessive paddling or flipping of the front feet. The animal may either hold the elbows out or tucked in and often stands with the feet rotated outward. DIAGNOSIS The routine monitoring for the presence of elbow dysplasia is carried out from a lateral x-ray of the flexed elbow joint taken when the dog is over 12 months of age. Correct radiograph technique is critical for making the diagnosis. ADVICE It is generally considered that dogs with grade 3 elbow dysplasia should not be used for breeding. And that dogs with grade 2 should be considered a serious risk.
These are Rodorbal Sweet As Candy's xrays. She has perfect scores of 0:0 elbows and 0/0 hips
Click here to view Candy's hip and elbow report under the AVA scheme: Candy's hip and elbow report Click here to view Gilly's hip and elbow report under the new CHEDS scheme: Gilly's hip and elbow report
|